Get the free silverscript mail order pharmacy
Show details
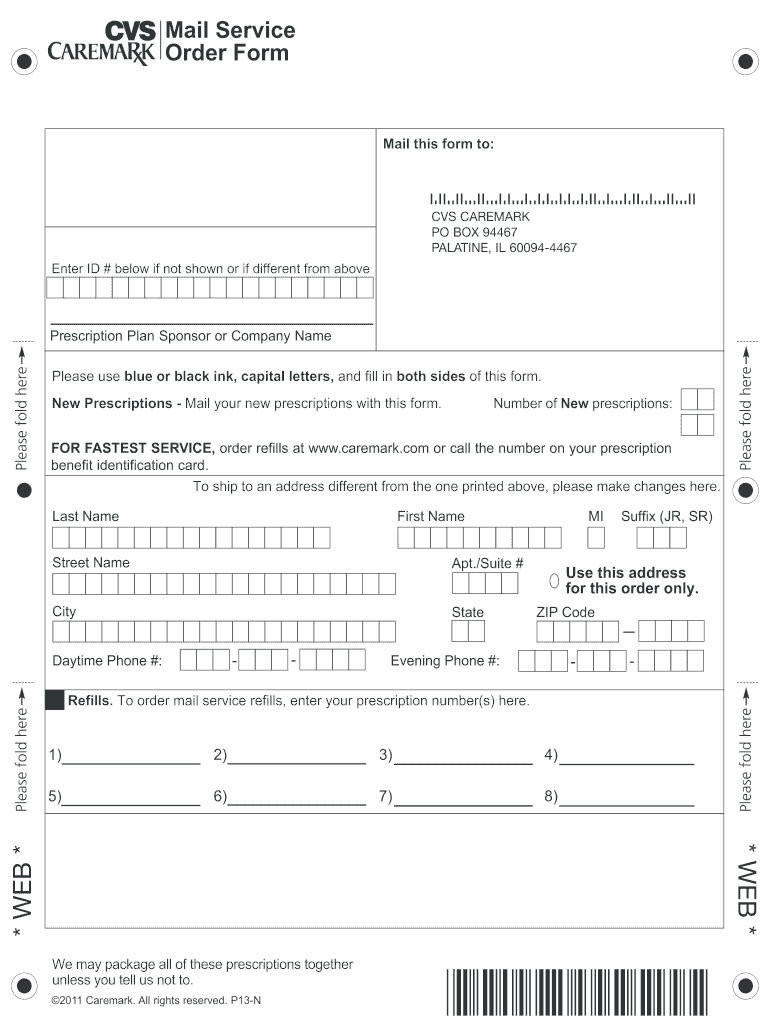
RESET FORM Mail Service Order Form PRINT FORM Mail this form to: CVS REMARK PO BOX 94467 PALATINE, IL 60094-4467 Enter ID # below if not shown or if different from above Prescription Plan Sponsor
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign silverscript mail order form
Edit your silverscript pharmacy form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your silverscriptonline com form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit silverscript pharmacy mail order online



Follow the steps down below to use a professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit silver script pharmacy form. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Save your file. Select it in the list of your records. Then, move the cursor to the right toolbar and choose one of the available exporting methods: save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out silverscript mail order is a lower cost and with convenience form
How to fill out silverscript mail order pharmacy:
01
Start by gathering all the necessary information and documents such as your prescription, insurance information, and personal details.
02
Visit the Silverscript website or call their customer service to initiate the mail order process.
03
Provide your personal information, including your name, address, and contact details.
04
Upload or provide the necessary prescription details, including the medication name, dosage, and quantity.
05
Submit any required insurance information, including your policy number and any applicable co-pay information.
06
Provide payment information for any out-of-pocket expenses, if applicable.
07
Review and confirm all the information you have provided to ensure accuracy and completeness.
08
Follow any additional instructions provided by Silverscript for submitting the order successfully.
09
Wait for confirmation from Silverscript regarding the status of your mail order pharmacy request.
Who needs silverscript mail order pharmacy:
01
Individuals who require long-term medications for chronic conditions and prefer the convenience of receiving them by mail.
02
People who have difficulty accessing local pharmacies or struggle with transportation to pick up their prescriptions.
03
Those who desire cost savings and potential discounts on medications through the mail order pharmacy service.
Fill
what is the best pharmacy to use with silverscript
: Try Risk Free
People Also Ask about silver script mail order
How do I make a mail order for a pharmacy?
Start an online pharmacy by following these 10 steps: Plan your Online Pharmacy. Form your Online Pharmacy into a Legal Entity. Register your Online Pharmacy for Taxes. Open a Business Bank Account & Credit Card. Set up Accounting for your Online Pharmacy. Get the Necessary Permits & Licenses for your Online Pharmacy.
Does SilverScript use express scripts?
pharmacy or through a mail-order pharmacy. The SilverScript network has most of the same retail pharmacies that are in your current Express Scripts Medicare network (CVS Pharmacy®, Costco, Duane Reade, Kinney Drug, Rite Aid, Walgreens, Walmart etc..)
What is the downside to mail order pharmacies?
Medication Errors. A mail order pharmacy doesn't know the patient as a local pharmacist may. This compounds the chance of error when a health care provider mistakenly writes down the wrong medication, dosage, or frequency (about 50% of medication errors).
Is mail order cheaper than pharmacy?
When you use a mail order pharmacy, you often pay a much smaller copay and may get a longer supply of the medication. Mail order pharmacies are often jointly owned and managed by the pharmacy benefit manager or Health Insurance Company that provides your coverage.
Does SilverScript use CVS?
SilverScript Insurance Company, a CVS Health Company, Introduces Three Medicare Prescription Drug Plan Options for 2019. We enter our 60th year as one of the most trusted brands in America.
Is Walgreens a SilverScript Preferred pharmacy?
Since 2021, Walgreens has focused on participation in preferred networks. For 2023, it will be preferred in nine plans. However, for 2023, Walgreens will be an out-of-network pharmacy for Aetna's SilverScript SmartSaver.
Is SilverScript and CVS Caremark the same?
SilverScript, administered by CVS Caremark, provides an Automatic Refill and Renewal program for home delivery, CVS Pharmacy Pickup and Delivery Options, CVS Specialty Pharmacy and over 66,000 pharmacies are available under the CVS Caremark network.
Can you use Walgreens with SilverScript?
Aetna is owned by CVS Health, so a SilverScript plan may be used at any CVS pharmacy. CVS is a preferred in-network pharmacy. Walgreens is a standard in-network pharmacy. While SilverScript plans may be used at Walgreens, the savings may not be as high as they would at a preferred in-network pharmacy such as CVS.
How do I set up a mail order prescription?
Ask your doctor to send your prescription directly to the mail order pharmacy. Or fill out an order form on the pharmacy's website and attach your prescription. Get your prescriptions delivered safely and conveniently to your doorstep. They'll usually come as a 90-day supply.
Does SilverScript use CVS Caremark?
SilverScript is an affiliate of CVS Caremark. Your new plan through SilverScript will be the only prescription drug plan for Medicare-eligible Retirees of MPIHP. Please watch your mail for additional information from SilverScript. Q: Will I be able to continue to use Express Scripts?
What is the difference between mail order and online pharmacy?
The main difference is that online pharmacies don't have brick-and-mortar locations that are accessible to the public. With a mail-order pharmacy, all communication between pharmacy staff, health care providers and customers is done over the phone, through text messaging or emails.
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I complete silver script com online?
With pdfFiller, you may easily complete and sign ask your doctor to send as a 90 day supply online. It lets you modify original PDF material, highlight, blackout, erase, and write text anywhere on a page, legally eSign your document, and do a lot more. Create a free account to handle professional papers online.
How do I fill out how to fill out silverscript 07 using my mobile device?
The pdfFiller mobile app makes it simple to design and fill out legal paperwork. Complete and sign silverscript and other papers using the app. Visit pdfFiller's website to learn more about the PDF editor's features.
How do I complete is silverscript and cvs caremark under the cvs caremark network on an Android device?
Complete silverscript administered by cvs caremark continue to use express scripts and other documents on your Android device with the pdfFiller app. The software allows you to modify information, eSign, annotate, and share files. You may view your papers from anywhere with an internet connection.
What is silverscript mail order?
Silverscript mail order is a pharmacy service that allows individuals to receive their prescription medications through the mail, typically at a lower cost and with convenience.
Who is required to file silverscript mail order?
Individuals enrolled in certain Medicare Part D plans, particularly those offered by Silverscript, are required to use the mail order service for their prescriptions as a condition of their plan.
How to fill out silverscript mail order?
To fill out Silverscript mail order, individuals must complete a mail order form provided by Silverscript, including their personal information, prescription details, and payment information before sending it to the pharmacy.
What is the purpose of silverscript mail order?
The purpose of Silverscript mail order is to provide a convenient and cost-effective way for patients to access their medications without needing to visit a pharmacy in person.
What information must be reported on silverscript mail order?
Required information includes the patient's name, address, phone number, insurance details, prescription medication name and dosage, physician's information, and payment information.
Fill out your silverscript mail order pharmacy online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Silverscript Mail Order Pharmacy Phone Number is not the form you're looking for?Search for another form here.
Keywords relevant to visit the silverscript website or initiate the mail order process text provide your personal information including
Related to silverscript com website








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
